Inflammation: The Root Cause Of Major Diseases.
Source: Thailand Medical News Oct 27, 2019 6 years, 5 months, 5 days, 23 hours, 26 minutes ago
Tons of medical research is showing that
chronic inflammation may be the common factor in many diseases. What is even more worrying is conditions known as
chronic inflammation and also prolonged low i
nflammation status which millions of individuals are walking around with not knowing the condition of their bodies and the detrimental effects it can have.
When considering ways for disease risk reduction, it often seems as though we need to keep a running tab of things to avoid or embrace.(and believe me research is showing that there are tons of things to avoid which can make life a bit boring!) Lay off saturated fats to keep our arteries clean. Steer clear of sugars and carbs to stave off diabetes. Stay away from smoking and air pollution to prevent lung cancer. Solve the sudoku puzzle to outwit dementia. And exercise, exercise, exercise! Wouldn't it be nice if there were a one-stop approach to health just as there is to shopping?
Despite the fact that there may never be such a single path, mounting evidence suggests a common underlying cause of major degenerative diseases. The four horsemen of the medical apocalypse ie coronary artery disease, diabetes, cancer, and Alzheimer's, are all riding the same steed:
inflammation.
Scientific research over the last two decades on
inflammation has created a shift in medical thinking. For two millennia it has been viewed mainly as a necessary, even beneficial, response to illness or injury. But now both observational studies and laboratory research are indicating that
inflammation can be more of a bane than boon, the common, causative factor in many diseases.
In medicine,
inflammation is part of the immune response. It's a process that depends both on the physical actions of white blood cells and the chemicals that they produce: antibodies, cytokines, and the like. Over the last several decades, scientists have identified dozens of new immunological and inflammatory molecules and the pathways through which they interact. The loops and feedbacks of those pathways mean inflammation can be turned on and off in any number of ways. The problem comes when it is left on, for no apparent reason.
Immunologists still describe
inflammation as dependent on two basic processes for simplicit sake.
The first, innate immunity, relies on granulocytes and complement. Granulocytes are short-lived white blood cells containing enzyme-filled granules that dissolve foreign substances. Complement is an array of circulating proteins produced in a cascade of enzymatic activity in the presence of microbes.
The other process, adaptive immunity, is directed specifically at microbes that have invaded the body previously. It's largely the responsibility of white blood cells called lymphocytes. T lymphocytes, or T cells, are the master strategists of the process, directing cells and chemicals to eradicate the invader. B lymphocytes,
or B cells, produce antibodies, which attach to specific pathogens and call in the complement to help dispatch the invader. Macrophages (literally "big eaters") are the scavengers, swooping in to eliminate the remains of microbes, dead granulocytes, and cellular debris created in the skirmish. While they clean up, macrophages also process information about individual pathogens and transmit it to the lymphocytes, which store the information for future reference.
As foreign pathogens are eliminated, suppressor T cells turn down the inflammatory response, so the regeneration of tissue injured either by the invader or by "friendly fire" from the immune system can begin. Fibroblasts, cells that produce collagen and fibrin, arrive to create a scaffold for new tissue cells. If the damage is extensive, fibrin and collagen may become thick enough to replace the original tissue and form a scar.
Roman physician Aurelius Cornelius Celsus described the four cardinal signs of inflammation —
calor (heat),
dolor (pain),
rubor (redness), and
tumor (swelling) — a Latin litany still learned by medical students today. But these symptoms are mainly tip-offs for acute inflammation.a nd these days is quite irrelevant.
Typically,
chronic inflammation often stays under the patient's and doctor's radar. It occurs when the triggering agent isn't entirely eliminated or the suppressor T cells don't call off the immune system after the body has repulsed the invasion.
All individuals have some level of
chronic inflammation slowly waging a war of attrition on tissues and organs, its activity often evidenced only in blood tests. But if it's turned up a notch or two,
chronic inflammation can wear away at the body so that the damage is devastating.
There is evidence of i
nflammation's sweeping, "cross-platform" effects. Observational studies, like the Framingham Heart Study and the Nurses' Health Study, have found lower rates of a number of degenerative diseases in people who take nonsteroidal anti-inflammatory drugs (NSAIDs) regularly usually for pain or arthritis. High levels of
C-reactive protein (
CRP), a marker for
inflammation, are associated with several illnesses.
Unforunately, our ideas about disease are organized by organ system, so scientists have tended to focus on the inflammatory process in particular organs or tissues. They are beginning to work out how
inflammation lays the groundwork for the following:
1. Inflammation and Coronary artery disease.
Cardiovascular research indicates that
inflammation acts in concert with an excess of "bad" LDL cholesterol to create atherosclerosis. At high blood levels, LDL cholesterol becomes oxidized. That makes it recognizable to the immune system and marks it for ingestion by macrophages. The lipid-loaded macrophages trigger complement activity that damages the vascular endothelium the layer of cells that lines the inside of blood vessels. Macrophages and their fatty cargo slip through the resulting cracks and lodge next to the arterial wall, where they are encased in a shell of fibrin and form arterial plaque. As the plaque grows and its fibrin coat is stressed, it may rupture, forming a clot that blocks a coronary artery supplying oxygen to the heart muscle. Heart tissue nourished by the artery then dies, causing a heart attack.
Clinical studies have determined that people whose CRP levels rank in the top third are twice as likely to have a heart attack as those with CRPs in the lowest third. The risk is even greater if a person also has high cholesterol. More doctors are adding a CRP test to the battery of routine screening tests for adults.
2. Inflammation and Diabetes.
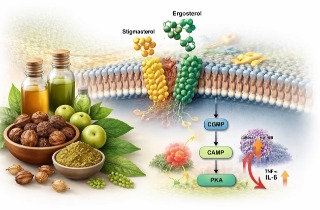
Numerous large observational studies have shown that people with high levels of CRP are more likely to develop insulin resistance, a precursor to full-fledged diabetes in which cells rebuff insulin and therefore don't properly metabolize glucose circulating in the blood. Researchers have also found that people who ultimately develop diabetes have high levels of inflammatory molecules, including TNF-α, a molecule produced by macrophages, and T cells.
TNF-α seems to increase the liver's production of glucose and triglycerides and interfere with insulin's duties as a blood sugar escort. Moreover, insulin has anti-inflammatory effects of its own. Thus inflammation not only sets the stage for insulin resistance but accelerates as insulin resistance sets in, which may further hasten the onset of diabetes.
3. Inflammation and Cancer.
Two centuries ago, the pathologist Rudolf Virchow termed cancer a "wound that doesn't heal." He noticed that tissue from malignant tumors contained high concentrations of inflammatory cells and hypothesized that the tumors often formed at sites of
chronic inflammation. Recent evidence suggests that he was right. About 22% of cancers including cancers of the liver, cervix, and stomach are closely linked to infectious diseases. Cigarette smoke and asbestos contain inflammatory substances. Exposure to cigarette smoke is a notorious cause of lung cancer, and exposure to asbestos is linked to mesothelioma, a cancer of the tissue lining the chest.
Laboratory research has shown that products of inflammatory reactions, such as reactive oxygen species, damage cellular DNA, creating mutant genes that lead to cancer. Macrophages, the mop-up molecules in the inflammatory process, churn out numerous tumor growth factors and appear to spur on angiogenesis, the growth of new blood vessels that nurture tumor cells with a fresh supply of blood. In short, malignant tissues seem to commandeer many of the inflammatory weapons sent out to vanquish them.
4. Inflammation and Alzheimer's disease.
Physicians once thought the central nervous system was outside the reach of the immune system. The blood/brain barrier, formed by tightened capillaries, acts like a bouncer, screening out inflammatory cells and molecules so they can't enter the brain. Yet observational studies have found links between NSAIDs (aspirin, ibuprofen, and naproxen), COX-2 inhibitors, and other anti-inflammatory medications and a lower risk of Alzheimer's disease. In addition, the brain may have its own branch of the immune system. Cells inside the brain called microglia, the counterparts to macrophages, swarm and engulf foreign substances and release TNF-α and other inflammatory molecules. Excess production of a molecule called beta-amyloid appears to play an important, and perhaps initiating, role in Alzheimer's disease, but the immune response may also be involved. Once microglia ingest beta-amyloid, they become enshrouded in fibrin and form the plaques characteristic of the disease.
Recent Developments With Regards To Inflammation
The topic
Inflammation is now a fertile field for basic research. The gene for selenoprotein S, a protein that plays a pivotal role in controlling inflammation, may lead to a test predicting who is at high risk for inflammatory disorders, and to the development of new drugs for
chronic inflammation.
Currently there are already scores of anti-inflammatory agents on the market, ranging from plain old aspirin to high-tech bioengineered molecules for treating asthma,
rheumatoid arthritis, and multiple sclerosis. Long-term use of NSAIDs is a balancing act, because while it may keep the fires of inflammation burning low, it can also cause stomach bleeding and liver and kidney damage. The COX-2 inhibitors, especially rofecoxib (Vioxx), have been linked to increased heart attack risk. Still, the daily 81-mg dose of aspirin recommended for people at high risk for heart attack is a safe bet.
Commonsense health practices may also help. Keep regular dental appointments to spot and treat periodontal disease; the evidence is mixed, but some research has sketched a possible link between gum disease and coronary artery disease. Take the full prescribed dose of antibiotics to prevent lingering infection and reinfection with resistant bacterial strains.
Low-calorie diets and moderate exercise remain the surest thing for preventing degenerative inflammatory disease. Obesity is linked to high CRP levels, as are "bad" fats and refined carbohydrates. Saturated and trans fats tend to stoke the immune response, while omega-3 fatty acids (in fish oils) and monounsaturated fats (such as olive and canola oils) may dampen it. Highly processed carbohydrates may promote
inflammation by aiding the formation of free radicals, so whole grains with unrefined carbs are more healthful. Alcohol in moderation only also cools off
inflammation.
New emerging research have also shown that besides processed foods, gut microbiome being destroyed, sexual promiscuity (by contraction of various STDs) even coffee drinking directly or indirectly are linked to causing
inflammation in the body.
Below is a link to ResearchGate’s list of clinical studies on
inflammation.
Thailand Medical News will be publishing a detailed article about detection of
chronic inflammation and ways to prevent it in a forthnights time.
References:
https://www.researchgate.net/journal/1023-3830_Inflammation_Research